Lis Franc Injuries – Langwarrin Podiatrist Brennan Jenkins discusses
The Lis Franc Injury is something we hear all too often and has been known to sideline some big names in the sporting world. Our very own podiatrist, Brennan Jenkins, discusses all things Lis Franc…..
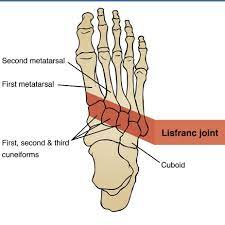
Anatomy and Function
The LisFranc joint is the collective name for the multiple joints that connect the base of the metatarsal bones to the cuneiform and cuboid bones, with special attention being paid to the articulation between the medial cuneiform and the base of the 2nd metatarsal. The LisFranc ligament is a combination of 3 individual ligaments: the dorsal LisFranc ligament, the interosseous LisFranc ligament and the plantar LisFranc ligament. Generally speaking, this is a very stable joint which acts to maintain proper alignment through the midfoot whilst acting to absorb shock through early – mid stance in the gait cycle.
{kind=link}
Mechanism of Injury
This traumatic injury requires large forces to be placed through the joint. Injuries can range from a mild sprain of one of the three LisFranc ligaments, to a fracture dislocation injury of the entire joint complex resulting in gross deformity of the midfoot. As the LisFranc joint is very stable, injuries to the joint are quite rare and complex, making up 0.2% of all fractures, however the diagnosis is missed 20% of the time (Trevino & Kodros, 1995). If this injury is missed in the acute presentation, it can lead to degenerative joint disease which can often occur from the trauma itself.
There are two main causes of the injury – either due to direct or indirect forces. Direct forces resulting in a LisFranc injury tend to result from large objects landing directly on top of the joint, such as a very heavy piece of furniture being dropped on top of the foot. Indirect forces which result in injury occur when there is an excessive plantarflexion and/or inversion moment of the forefoot on the rearfoot, resulting in excessive twisting.
Assessment
An in-depth patient history should be taken, determining the mechanism of injury, level of force which was applied to the foot and the patient’s level of pain. X-Rays are often able to detect significant LisFranc injuries. If X-Rays return unremarkable yet there is still clinical suspicion, MRI is known to be the most sensitive imaging modality for diagnosis of LisFranc injuries. Due to the small size and overlying nature of the ligaments, ultrasound is unable to provide an accurate diagnosis of this injury.
Clinically, the patient will often present in significant pain with difficulty weightbearing. There will regularly be significant bruising in the medial longitudinal arch and pain on palpation of the 2nd metatarsocuneiform joint. The piano key test can be utilised to assess injury by stabilising the hindfoot and midfoot, while placing a plantarflexion force to the metatarsal head. A positive test result would produce pain at the respective metatarsocuneiform joint.
Treatment
Treatments can range from conservative treatment for mild sprains via reduced activity levels and the use of a custom foot orthosis to support the midfoot to maintain medial arch integrity and optimise foot function. More severe cases will require require surgery with open reduction internal fixation performed most regularly at the 2nd metatarsocuneiform joint; this, however, can involve all of the midtarsal/LisFranc joints depending on the region of injury.
Depending on the severity of the injury a period of immobilisation and non-weight bearing is required. The patient then begins a gradual return to weight bearing whilst wearing a CAM walker over 6 weeks with customised medial arch orthoses in situ. A gradual and progressive rehabilitation program will be written for the patient, beginning at the removal of the below-knee cast. This will include strengthening of the intrinsic foot musculature, calf and also proximal strengthening at the hip joint. Orthoses will then be required post-operatively for at least 12 months (and often indefinitely) to maintain medial arch integrity and optimise foot foot function.
Our team of podiatrists at Footlab Plus have extensive experience in assessing, diagnosing and rehabilitating Lis Franc injuries and work closely alongside surgeons to optimise recovery
Want to know more or get in touch click here
References
Trevino, S.G. & Kodros, S., 1995. Controversies in tarsometatarsal injuries. Ortho Clin North Am 26, pp.229-238